Sort of. To my understanding, there's one committee, the Vaccines and Related Biological Products Advisory Committee, that oversees this stuff and the meetings are kind of sporadic. They're
meeting on the 17th about the booster doses and
then again on the 30th to talk about a bunch of stuff I don't understand and flu shots. After that, they don't have anything on the books for
the rest of the year. This isn't to say they can't call another meeting, but it's still a government agency and all the red tape that goes along with it.
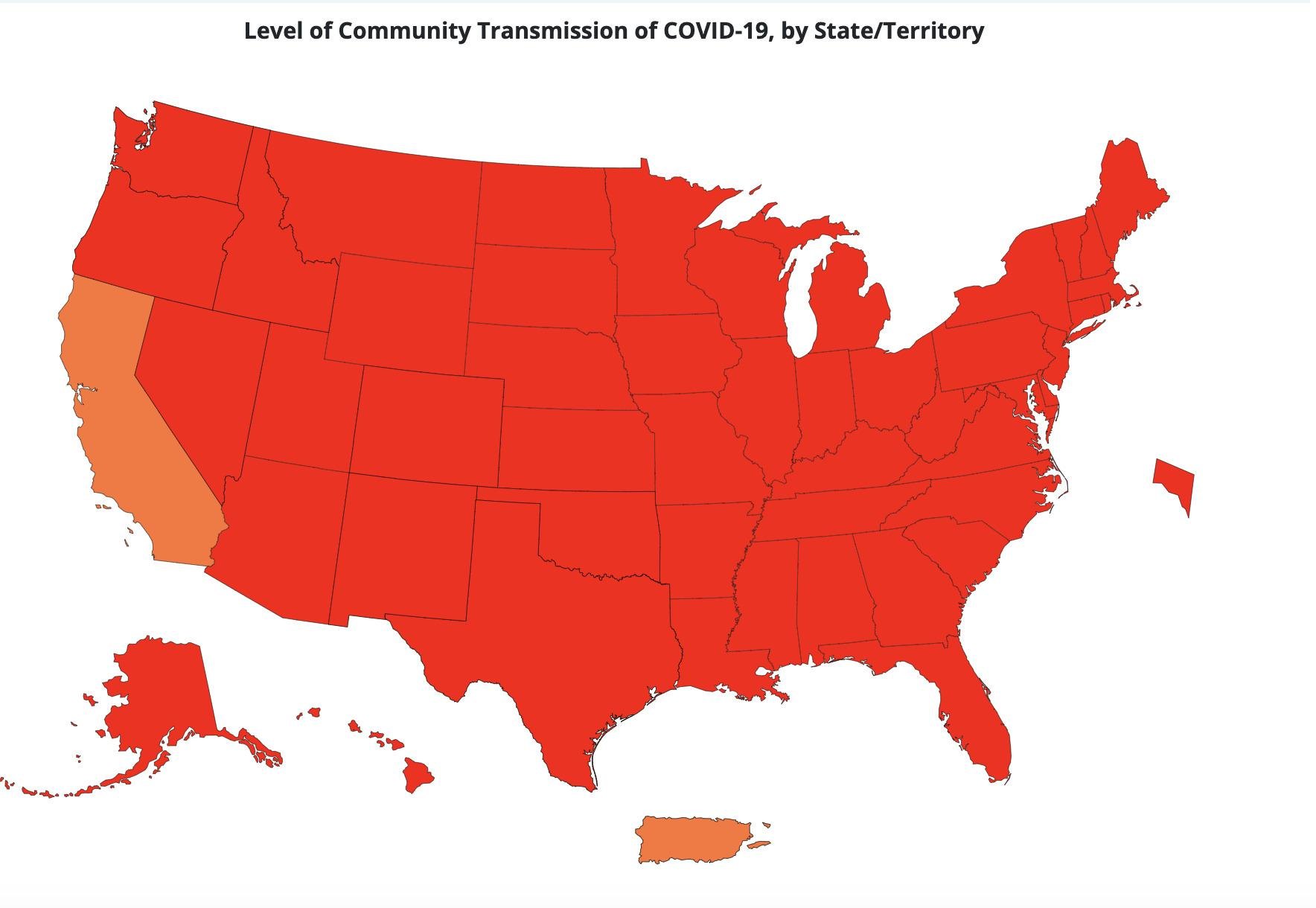
Also, if they don't have a meeting prior to Thanksgiving, I suspect there won't be one until after the start of 2022. By then, kids will have had a really rough go of it. In Utah alone, we're seeing 400-500 pediatric cases a day and that's just what's been tested and reported. It's more likely we're seeing 1,000+ pediatric cases a day and our PICU is completely full and has been for a couple of weeks now. Couple this with a higher than expected RSV and flu season, and well, you can see where it gets dicey. Assuming we're at 1,000 cases per day for kids and we have roughly 250,000 kids ages under 12 in Utah, it's likely that a portion of them have already gotten COVID or have immunities from their mother. So let's say it's 200,000, which means we'd burn through the entire population by April 2nd at this rate.
It's honestly ludicrous that the vaccine wasn't rolled out for kids prior to the start of school. It's the FDA's fault too since after the data was submitted by Pfizer and Moderna, the
FDA asked them in July to provide more data, which effectively started the process over again. They typically need six months' worth of data too, so even if they started immediately, that puts us at January at the earliest. However, after the data is submitted, we need to wait for the committee to convene, go over the data, and issue a EUA. This process can take upwards of six weeks. So now we're at the end of February/beginning of March at the earliest. This is also assuming that the trials started in July, which they didn't because as of last month they were still recruiting. So using Utah as an example, we're on track for the entire population of ineligible kids to get COVID before they can be fully vaccinated.
The
American Academy of Pediatrics is pretty fed up with it too.
What the FDA needs to do is approve EAU for kids, publish the data, and let parents make the decision along with their kid's pediatrician. I would 100% get my nearly 3-year-old son vaccinated immediately if this was the case, like make an appointment with his doctor the same day as approval kind of immediately. I know his doctor would be on board too since she's very pro-vaccine and won't take kids on as patients if they don't follow the vaccine schedule, which is something I appreciate.
Schools shouldn't mandate it until it's fully approved though. So really for the 2022-2023 school year, the COVID vaccine should be a requirement for your kid to attend school.


www.cnbc.com




")