It was also last in healthcare outcomes, arguably the most important metric for a healthcare system.
Which makes me wonder why the US system is defended so fervently by some Americans. I understand their distrust in government, but there's really only one direction you can go from being last....
From what I understand it's "last" largely because of uninsured, or underinsured poor people (& the general unhealthiness of a lot of the American population). Lop those people off the system & it performs much better, which is why it ends up being a "class warfare" issue ... & by extension a race issue.
In the US, the health care system has operated on a for-profit basis. Therefore health care must be paid for. You don't have to be employed to get health care. You merely must pay for it. There is Medicare for those over 65. Disability health care payments are available for those that need it. Retired military have their own system, etc. Free government health care is not provided in the current US system. For that to happen, dramatic changes would have to happen. The few candidates for office who have proposed that haven't gotten very far. Bernie Sanders took the idea as far as he could, but was labeled as a socialist or worse and rejected by the Democratic party.
Disability health care payments are available for those that need it. Retired military have their own system, etc. Free government health care is not provided in the current US system.
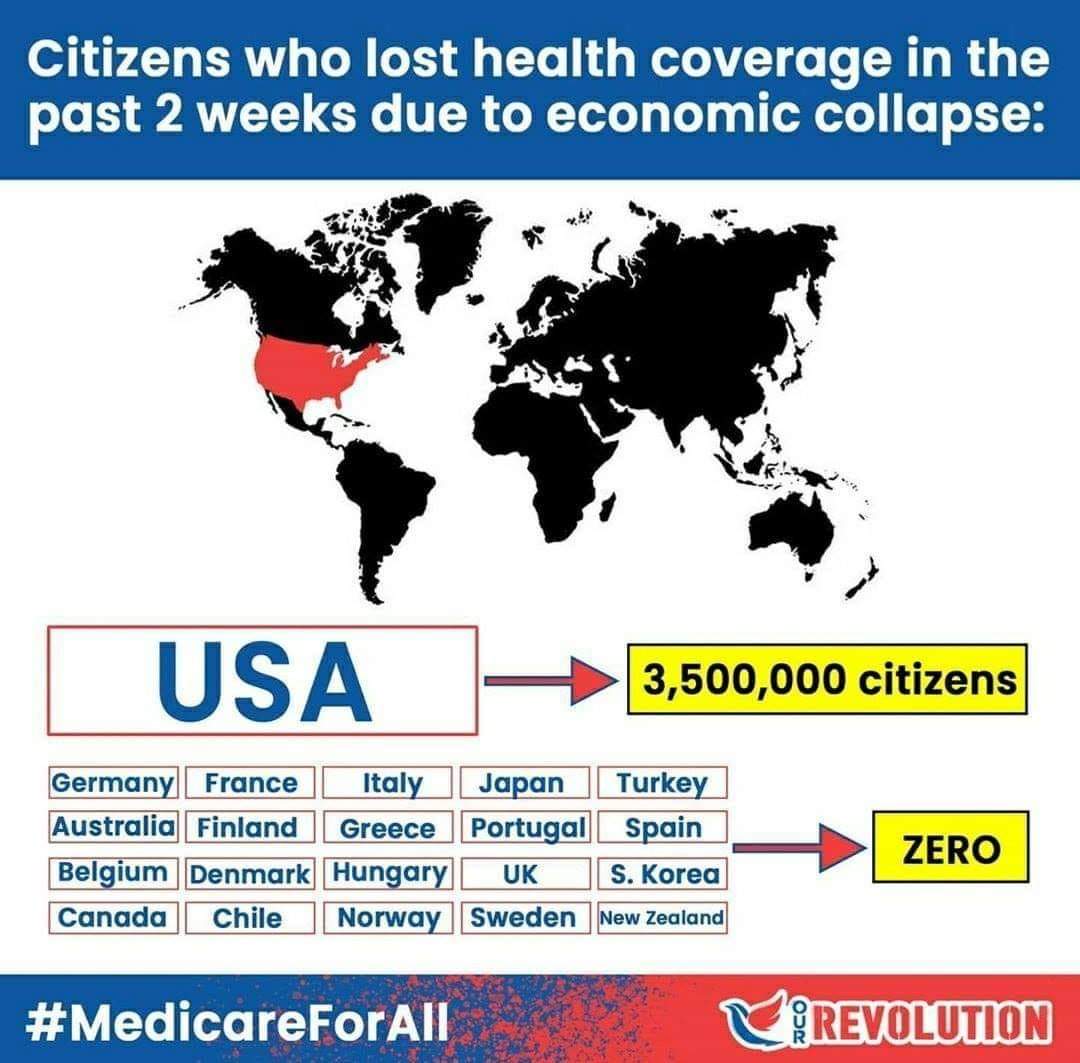
I was honestly on the fence about nationalized healthcare but this event has really demonstrated how the private healthcare system is a giant Achilles heel to our economy and not just our way of life. Private medicine just doesn't work and whenever it fails (which is apparently during any crisis) FEMA has to fly in and save the day anyways.
I was honestly on the fence about nationalized healthcare but this event has really demonstrated how the private healthcare system is a giant Achilles heel to our economy and not just our way of life. Private medicine just doesn't work and whenever it fails (which is apparently during any crisis) FEMA has to fly in and save the day anyways.
A regional healthcare provider can't mobilize a response to something like this. They always require federal support to rapidly expand and deal with a crisis. How does money change hands in situations like this? It's our money being muddled with the private sector and they'll still try to send you a bill when it's all over. The whole thing is a mess.
A regional healthcare provider can't mobilize a response to something like this. They always require federal support to rapidly expand and deal with a crisis. How does money change hands in situations like this? It's our money being muddled with the private sector and they'll still try to send you a bill when it's all over. The whole thing is a mess.
If I'm jumping to the conclusion, it sounds like you're maybe dissatisfied with Medicaid. I'm not entirely sure. I was thinking along the lines of the US being all over the vaccine race, and the US death statistics substantially lagging the case statistics when compared to many countries with Universal Healthcare. So for example, something like this:
It's problematic, the statistics are hard to suss out because in the US we primarily test only the more severe COVID-19 cases. Lots of people are (or were) being told that unless their symptoms are severe, they don't get a test. You might see that alone as a failing (and it is), but our healthcare system seems to be doing a pretty fantastic job of keeping the death rates low for cases that we know about (many of which are severe).
It's problematic, the statistics are hard to suss out because in the US we primarily test only the more severe COVID-19 cases. Lots of people are (or were) being told that unless their symptoms are severe, they don't get a test. You might see that alone as a failing (and it is), but our healthcare system seems to be doing a pretty fantastic job of keeping the death rates low for cases that we know about (many of which are severe).
The issue isn't solely based on fatality rates. People are going to get billed, as much as $75,000 depending on the care they received. This disease statistically afflicts poorer people greater so this is going to be a huge problem because they're not going to pay those ridiculous bills. Costs are going to be kicked forward to paid insurers next enrollment period.
7 women at my work got knocked up in the same year and just that shot our insurance rate up. What do you think is going to happen to our rate after this? The insurance company doesn't like taking financial losses and those thousands of uninsured patients and thousands of dead patients will have their costs covered by us.
Specifically you mean that hospital billing and insurance entanglement is a joke... right? Because there's a lot to the "system" that goes beyond that.
If I'm jumping to the conclusion, it sounds like you're maybe dissatisfied with Medicaid. I'm not entirely sure. I was thinking along the lines of the US being all over the vaccine race, and the US death statistics substantially lagging the case statistics when compared to many countries with Universal Healthcare. So for example, something like this:
It's problematic, the statistics are hard to suss out because in the US we primarily test only the more severe COVID-19 cases. Lots of people are (or were) being told that unless their symptoms are severe, they don't get a test. You might see that alone as a failing (and it is), but our healthcare system seems to be doing a pretty fantastic job of keeping the death rates low for cases that we know about (many of which are severe).
As you've mentioned it's very hard to suss out when comparing different countries because of the different testing and different ways of recording deaths, so is it really relevant to how healthcare systems compare?
There also seems to be far more at play than just health systems as well. In the US you have huge variances from state to state. I wouldn't think the hospitals vary that much, would they?
For example:
As of Monday (April 13), New York's death rate linked to COVID-19 was 513 deaths per million people, compared with California's 17 deaths per million. With more than 70% of the state's related deaths being reported in New York City, it begs the question: Is there something about the city's five boroughs that is boosting transmission and fatalities?
As you've mentioned it's very hard to suss out when comparing different countries because of the different testing and different ways of recording deaths, so is it really relevant to how healthcare systems compare?
There also seems to be far more at play than just health systems as well. In the US you have huge variances from state to state. I wouldn't think the hospitals vary that much, would they?
There is a lot of variation between the states. But in general the US seems to be a doing a good job of keeping mortality low. For as much crap as our healthcare system gets, we seem to be holding our own. There are plenty of social factors that plant the US as one of the worst for case transmission, and we do have the most cases of any nation in the world. Yet we're keeping mortality fairly low while not testing low risk cases. I think that's commendable. If you think that's somehow unfair to other nations, you're not reading me right.
There is a lot of variation between the states. But in general the US seems to be a doing a good job of keeping mortality low. For as much crap as our healthcare system gets, we seem to be holding our own. There are plenty of social factors that plant the US as one of the worst for case transmission, and we do have the most cases of any nation in the world. Yet we're keeping mortality fairly low while not testing low risk cases. I think that's commendable. If you think that's somehow unfair to other nations, you're not reading me right.
Yes, the US does seem to be holding it's own... everywhere but New York, which acquired it's high rate in much the same way as the Euro countries did. This is why I think it's irrelevant to compare these numbers for Health Care system comparison purposes. There's just way too many variables in the way Covid-19 was introduced to each country, or even parts of each country in the US's case.
Hospitals can vary wildly. Typically, we look at something called Quality Measures to see just how good or bad a hospital is. They're not all-encompassing, but they do measure things like patient safety, mortality, readmissions, and effectiveness of care. There are also several accreditation firms that will come in and certify a hospital and tell them how to improve, the most common is The Joint Commission. The government also measures this sort of stuff through CMS, which performs audits on hospitals and their finding will affect a hospital's Medicaid/Medicare reimbursements.
Off the top of my head, I think New York has the most hospitals with a low-quality score while Massachusetts has some of the best. Overall, the south has some of the worst healthcare and the northeast has some of the best with the rocky mountain region coming up right behind it.
Yes, the US does seem to be holding it's own... everywhere but New York, which acquired it's high rate in much the same way as the Euro countries did. This is why I think it's irrelevant to compare these numbers for Health Care system comparison purposes. There's just way too many variables in the way Covid-19 was introduced to each country, or even parts of each country in the US's case.
By your figures from above Belgium (the worst Euro death rate) has 34.17 per 100k *Edit: Correction, it's Spain with 38 deaths per 100k, New York has 51.3 per 100k. California on the other hand is doing far better (1.7 per 100k).
but our healthcare system seems to be doing a pretty fantastic job of keeping the death rates low for cases that we know about (many of which are severe).
and the US death statistics substantially lagging the case statistics when compared to many countries with Universal Healthcare. So for example, something like this:
This is pointless to compare with regards to Healthcare systems. The circumstances for each country, and even state to state (as I have shown above) are far too different.
This is pointless to compare with regards to Healthcare systems. The circumstances for each country, and even state to state (as I have shown above) are far too different.
The Death Rates don't tell the full story of a healthcare System though, multiple strands of the virus are forming and with variable danger levels so the Death Rate on many levels are out of each countries hands.
It also depends on the age demographic of a region, I would Imagine if Flordia was hit as hard as New York the Deathrate would sky rocket simply because of the age demographic.
but our healthcare system seems to be doing a pretty fantastic job of keeping the death rates low for cases that we know about (many of which are severe).
The highlighted part is what I've been referring to... and your use of that chart in post #1455 as a comparison of the US Healthcare system to the Universal Healthcare countries.... which is a flawed comparison due to many, many reasons.
Also, compared to the world death rate per 100k people you're really not doing that well in the US unfortunately.
The Death Rates don't tell the full story of a healthcare System though, multiple strands of the virus are forming and with variable danger levels so the Death Rate on many levels are out of each countries hands.
It also depends on the age demographic of a region, I would Imagine if Flordia was hit as hard as New York the Deathrate would sky rocket simply because of the age demographic.
The highlighted part is what I've been referring to... and your use of that chart in post #1455 as a comparison of the US Healthcare system to the Universal Healthcare countries.... which is a flawed comparison due to many, many reasons.
Yea, so I did mention that the spread was expected to be bad for a lot of reasons in the US. That's not really something the healthcare system can do anything about. Our healthcare system is not responsible for stopping the spread of the virus. And we have spread it quite extensively in the US. Which is why we lead the world in death and cases. Also why we'd lead the world in death per capita. This is not a measure of healthcare, this is a measure of social transmission.
What the US is doing well with is keeping the death rate low from cases. We have tons more cases than we know about, most of them benign. If anything our testing is more severely biased toward extreme cases than most other countries, and yet we keep our death rates from cases low.
Don't get confused between deaths per capita and death rate from coronavirus cases. Both are rates, but one is more decidedly aimed at healthcare.
I agree that there are a lot of complicating factors, such as demographics. Italy's population seemed to have a lot of older smokers, for example, which explains (in part) why their healthcare system got overrun. That's not particularly down to their healthcare system (although you might have expected a centrally planned system to be more prepared for overrun than say... a free market system), it's not the healthcare system's job to keep people from smoking or make sure they have enough babies. I'm not saying Italy did a bad job. In fact, I'm not saying anyone is doing a particularly bad job with death rate.
I'm saying the US seems to be doing a good job, with relatively low death rates (except for New York as you noted). This is partly down to our healthcare system doing well with cases. If we had a crap healthcare system, you'd expect high death rates.
Edit:
Incidentally, I get nothing but hit over the head with weaker more simplified statistics about how the US healthcare system is crap. Then suddenly when it does well in rather pertinent statistics, suddenly there's all this rigor that goes into how you can't compare.
Nonsense. We're doing well with coronavirus death rates (except for New York).
I believe Michigan is doing worse than New York. Based on what I've been able to see the mortality rate in New York is 6.55% and in Michigan, it's 6.85%. In talking with my parents and my inlaws it's pretty easy to see why Michigan is doing so poorly too. They simply aren't testing anyone and they're being told: "you're not sick enough". My sister-in-law was suspected to have COVID-19 and it took her two weeks before she could get a prescription for a test. Then when she went to schedule the test, she had to wait 4 days before a time slot was available at a drive-thru. After that, she had to wait 5 days before getting her results. So it took her a little over 3 weeks from when she had symptoms until she got her results. The test came back negative, but she still believes she had it and it'd just run its course.
By comparison, Utah has gotten to the point where we're testing people with no symptoms at all. If you want a test for any reason, you call a number and get a time slot at a drive-thru clinic. The lag is about an hour around SLC and around four hours in Summit County (Park City). Results are said to take anywhere from 24-48 hours, but most people get theirs back in less than six hours. I know other states are doing this as well and it certainly helps with the numbers and keeping things contained.
It also doesn't help that Michigan's governor half-assed the lockdown order. For whatever reason, she banned the sale of "non-essential items" but failed to explain what that meant. I've seen more than one person post pictures on Facebook from their local Target or Wal-Mart that shows baby items being deemed non-essential (apparently formula is the only thing you could buy). You also can't buy things like garden seeds, toys, games, outdoor equipment, and so on. Pretty much stores took her order as "only buy food", but that's not what it really meant at all.
On top of all this, Michigan has some of the best healthcare systems in the nation and, I believe, four of the largest as well. Unfortunately, because the governor got into a pissing contest with Trump and then failed to fill out the emergency declaration documentation correctly, there was a lag in federal help. This meant they ran out of PPE almost instantly and as a result, there's something like 700-1000 healthcare workers who have COVID-19 at just two hospitals.
It shocks me at just how bad a handful of states are doing, while so many others are maintaining their numbers, keeping the mortality rate low, testing thousands of people, and even keeping people out of the ICU if they're hospitalized.
I suggest there are two measures that might be used to rate healthcare re. COVID-19.
First, deaths per hospital admission, using a delayed figure for the admissions. I have a feeling that this number will be broadly similar for most countries where the hospitals don't get overloaded (and differences could be explained by factors other than care e.g. age, prevalence of smoking, obesity, etc).
Second, the number of COVID-19 deaths outside hospital as a percentage of all COVID-19 deaths. This might shed some light on the availability or standard of care outside hospital.
Neither of these stats has been readily available, in comparable ways, for many countries.
Deaths per cases mostly depends on how many tests are being carried out, and it seems US as a whole is doing relatively well on testing (undoubtedly better in some states than others). This chart gives some idea, although what isn't clear is how many people are tested (since some have multiple tests) or how localized testing is.
Yea, so I did mention that the spread was expected to be bad for a lot of reasons in the US. That's not really something the healthcare system can do anything about. Our healthcare system is not responsible for stopping the spread of the virus. And we have spread it quite extensively in the US. Which is why we lead the world in death and cases. Also why we'd lead the world in death per capita. This is not a measure of healthcare, this is a measure of social transmission.
This is what I've been saying all along. It wasn't me that first used death rates/statistics to compare Healthcare systems. I have said multiple times it can't be used to compare, not that the US system is worse, not that Universal Healthcare is better, just that using death rates to compare is flawed... that's all.
*snip* the US death statistics substantially lagging the case statistics when compared to many countries with Universal Healthcare. So for example, something like this: